By Nigel S.B. Rawson and John Adams
July 24, 2025
There are about 11,000 known rare diseases (Rare-X 2022), with more likely to be found. Despite individually affecting anywhere from fewer than a hundred to a few thousand people, these diseases impact three million Canadians. Many of the illnesses have a genetic cause, but the exact origin remains unknown for others.
Regardless of cause, Canadians living with rare diseases face difficult burdens – higher medical needs, increased suffering from mental or physical impairments, and caregiver assistance requirements; further, they often miss work, are forced to retire early, and face premature death. In addition, they must deal with the indirect costs associated with productivity losses and the non-medical costs related to modifications of lifestyle, homes, or vehicles. The estimated total economic burden of just 379 rare diseases in the United States in 2019 was US$997 billion (Yang et al. 2022). Direct medical costs and indirect costs from productivity loss accounted for 45 and 44 per cent of that total, respectively, while non-medical costs were seven per cent and health care costs not covered by insurance were another four per cent. US data are not directly transferrable to Canada due to differences in health care, but they suggest that the economic burden of rare diseases is significant for Canadian patients, unpaid family caregivers, our health care system, and society as a whole.
For decades, practitioners could do little to treat most rare diseases; the only options for patients were symptom relief and palliative care. Medical professionals commonly called these illnesses orphan diseases because clinical science often didn’t know how to categorize them within traditional disease hierarchies or know how to treat them. Pharmaceutical companies generally saw no business case to develop medicines for them, unless as a spinoff of research leading to development of therapy for a more common disorder. Health Canada conspicuously avoids using the term “orphan drugs.” Instead, it uses the anodyne phrase “drugs for rare disorders” (DRDs).
In the last 40 years, more DRDs have been created, with the rate of development accelerating since the US enacted the world’s first Orphan Drug Act in 1983. This act unlocked innovation by introducing incentives designed to stimulate research and develop small-market medicines. Those incentives included offering tax credits for qualifying clinical trials and providing exemptions from regulatory fees, as well as potentially giving the developer seven years of market exclusivity after approval regardless of patent or data protections. The act succeeded in its objective. In 1983, the US approved only 38 specific orphan drugs, but between 1983 and 2019, more than 5,000 received approval (Miller, Fermaglich, and Maynard 2021). This has made a dramatic difference for people living with about 600 rare diseases.
Mapping the human genome, first completed in 2003, is another factor that has stimulated the development of orphan drugs. Gene, cell, and tissue therapies now offer significant advances for some rare diseases (Chancellor et al. 2023; Lapteva et al. 2020; Weber, Maus, and Mackall 2020).
Following US leadership, many countries enacted orphan drug laws and developed rare disease strategies (Gentilini, Neez, and Wong-Rieger 2025), but Canada has not, despite patient advocacy groups such as the Canadian Organization for Rare Disorders (CORD) pushing for governments to do so (CORD 2015) and the World Health Organization stating that rare diseases are a priority for member states (WHO 2025). Canada continues to freeload on efforts in the US, Europe, and elsewhere. As a result, Canadian patients do without as fewer DRDs are launched in Canada than in the US or the European Union (Rawson 2018; Ward et al. 2022).
Although access to new DRDs is crucial to relieve suffering, improve productivity, and extend lives, a national rare disease strategy must encompass more than access to medicines. It should include improvements in screening for diseases in newborn infants, referral to accessible centres of clinical excellence, equitable access to timely diagnosis and treatment of rare diseases in patients of all ages, sustainable access to new drugs, policies to encourage innovative research, and pan-Canadian collection of data on rare diseases and their treatments, as well as the reduction or elimination of government/agency filing fees, gatekeeping burdens, and overlapping processes.
Let’s look at each item needed for a comprehensive strategy.
Newborn screening
A critical component of any national strategy to detect rare disorders is a wide-ranging approach to the screening of newborn infants. Many disorders manifest in early childhood and, even if they can’t yet be treated, it is important that diagnosis occurs as early as possible to assist with timely and appropriate access to support and treatments, and to give scientists a deeper understanding of the disorders. Early diagnosis is a building block to understanding the natural history of thus far untreatable disease and helps to drive research, funding, and policy attention to addressing unmet needs.
Like other elements of health care systems in Canada, newborn screening programs are established and funded by individual provinces and territories, with each having its own decision-making processes and policies. There has been little to no federal participation, let alone leadership, in addressing newborn screening. As new knowledge and technologies emerge, screening programs must update and expand.
Comparing the number of screened conditions across provincial and territorial programs is challenging due to differences in how the various conditions are defined and reported. Discrepancies in terminology add complexity to comparisons because different jurisdictions refer to and define screened disorders in different ways. Nevertheless, a 2015 examination of newborn screening around the world demonstrated reasonable consistency across American states, but the US screens for more diseases than Canada, which has considerable variation between provinces and territories (Therrell et al. 2015). This patchwork starts with the absence of a definition of “rare.” It is unsurprising that a type of “postal code lottery” exists for newborns as to who gets screened for what across Canada.
In 2016, Canada’s Drug Agency (CDA) recommended to the country’s ministers of health a pan-Canadian list of 22 conditions for which newborns should be screened (CDA 2024), but not all jurisdictions universally accepted the list. More recently, in 2024, an advisory panel appointed by the CDA expanded the list to 25 conditions by dividing one of the original 22 into three and it identified another nine requiring further review (CDA 2025). Harmonization in testing would provide fairness and consistency across Canada and the modest proposed extension would cost relatively little.
Access to timely diagnosis
As the name implies, rare diseases affect a small number of individuals. This means that individual clinicians see few to no patients with rare diseases in their career. Many general practitioners (80 per cent) and pediatricians (62 per cent) are not aware of or informed about rare diseases, so the understanding and clinical expertise needed to treat these diseases is limited and fragmented (CORD 2023). The lack of experience and absence of newborn screening for more disorders means individuals are commonly misdiagnosed (about 60 per cent initially receive an incorrect diagnosis) and endure a lengthy and costly odyssey until a correct diagnosis is made (Dragojlovic et al. 2020; Esquivel-Sada and Nguyen 2018; Glaubitz et al. 2025). On average, 4.8 years elapse before a patient receives a correct diagnosis for a rare disease in Canada, with some patients waiting much longer. Many see numerous health care providers at considerable expense before receiving a final diagnosis (CORD 2023). The cost of diagnosing can reach $6,300 per patient (Khure Health 2025). Using a BC study and assuming (as is frequently done) that one in 12 Canadians is affected by a rare disease, the financial impact of the diagnostic process on the health care system has been estimated at $19.7 billion over the 4.8 years.
Delays in diagnosis cause delays in access to appropriate care, leading to increased morbidity, poorer quality and/or loss of life, and increased costs to patients and their families, the health care system and the broader economy and society. Delays and incorrect diagnoses contribute to the progression of a disease before effective treatment can begin and can harm the mental health and well-being of patients and their caregivers.
These issues require improving the education of health care providers on rare diseases and establishing centres of excellence on rare disorders to provide more complete diagnosis and care for patients and their families and to generate and support research, produce and implement clinical practice guidelines, deliver professional and patient education to general practitioners and the public, and develop extended diagnostic, clinical, and educational services. Centres should work globally with other scientists and manufacturers to support existing rare disease registries and create new ones with an objective of improving patient care. While the focus of the centres of excellence would be rare diseases, discoveries the centres make could lead to significant advances in scientific knowledge benefitting the treatment of more common conditions and offsetting their establishment and running costs. For example, research into exceedingly rare congenital leptin deficiency led to greater understanding of the underlying processes of overweight and obesity (Reid 2016).
Although 85 per cent of rare diseases have a genetic cause, genetic testing and counselling is limited in Canada and, consequently, management of these disorders is often slow and poor. In a recent survey of Canadians with a rare genetic disease, only 44 per cent reported receiving screening, testing, and counselling, 43 per cent post-diagnosis support, 39 per cent newborn screening and testing, 36 per cent timely diagnosis, information, and counselling support, 22 per cent prenatal education and screening, and 16 per cent prenatal counselling, information, and support prior to pregnancy or delivery (CORD 2023). A need for increased access to screening, testing, and counselling for rare genetic diseases clearly exists in Canada, not just for the benefit of sufferers but also to reduce wasteful spending in diagnosing. The lack of a comprehensive strategy remains a barrier to addressing these problems.
Access to medicines and clinical care
There are many gaps in access to appropriate treatment for rare disorders in Canada. Among these are lack of access to care coordinators (63 per cent), counselling support at the time of diagnosis (74 per cent), and emotional and psychosocial support (70 per cent) (CORD 2023). These figures are from a Canada-wide survey and are, therefore, averages. Access to care and medicines varies widely across jurisdictions (Rawson and Adams 2024; Awada 2025).
There are 14 separate government drug plans that control the accessibility of new medicines. This requires drug developers to pass through at least five sets of gatekeepers (Rawson and Adams 2025), including Health Canada’s efficacy and safety review, health technology assessments that evaluate the “cost-effectiveness” of new medicines, negotiations between drug developers and the federal, provincial, and territorial governments’ price bargaining organization known as the pan-Canadian Pharmaceutical Alliance (pCPA), and further negotiations between developers and administrators of the individual government drug plans before they decide whether to list a drug. These processes not only take time and incur expense (Rawson and Adams 2024) but also have many flaws. Together, they stifle innovation by deterring developers, especially small start-ups, which are often the sources of innovative DRDs, from bringing their products to Canada before launching in many other countries (Rawson 2018; Ward et al. 2022).
Even when developers can successfully weave their way through these gatekeepers and have their DRDs listed in government drug plans, patients may not be able to access them. In a recent survey, 68 per cent of rare disease sufferers knew that Health Canada has approved a drug for their disease, but 49 per cent reported difficulty accessing the DRDs they need, with 36 per cent unable to access those medicines because the costs or co-payments are too high (CORD 2023). Rare disease sufferers are commonly unaware that, although an appropriate DRD might be listed in their government drug plan, access to it is restricted by the cost of co-payments and/or deductions or highly specific clinical or laboratory measurements that must be complied with before access is possible (Rawson and Vanstone 2021; Begovic 2022). Some restrictions on government drug plan access are explicit, but many are non-transparent, so that patients and clinicians can’t assess whether conditions are applied appropriately or equitably.
Costs of drugs for rare disorders
The per-patient cost for DRDs is frequently high. In a brief to the Standing Committee on Health (2019), the pCPA stated that current list prices for DRDs range from $500,000 to $4.9 million per person per year. The brief also said that “governments … face difficulties justifying spending funds on the reimbursement of these drugs when there is limited evidence showing that they offer significant health benefits.” This begs the question of what evidence these processes are willing to consider and appears to suggest, perhaps unintentionally, that the processes of Health Canada, the CDA, and the pCPA add little value in delivering beneficial DRDs, in which case the question arises as to whether we need these agencies, at least as they operate at present.
As many other reports do, the pCPA’s statement on the per-patient cost is based on the manufacturer’s list price, which is not the same as the much lower price that governments, through the pCPA, negotiate. Negotiated prices are confidential but based on available evidence are thought to be around 30 per cent less than the list price.
The focus on potential per-patient prices ignores the fact that for many rare diseases there are only a small number of patients and, consequently, the overall costs to the health care system – estimated to be about $19 billion in 2025 (Lech et al. 2022) – are a fraction of the $372 billion the government spends on health care (CIHI 2024).
Many find the prices of DRDs to be unacceptable because they believe drug developers charge high prices to make excessive profits. Developers charge high prices because most potential DRDs don’t make it to market due to a lack of efficacy or safety issues, while those that do have high costs of research, development, manufacturing, and regulatory compliance – and will only be used by a small number of patients from whom the developers must recoup those costs (Sabatini and Chalmers 2023).
There is also the view that, instead of paying thousands of dollars for a DRD for one person, the money could be used to pay for less expensive therapies for many more patients. However, despite health care funding being allocated on a population basis, care is and should be delivered as needed, not rationed per capita. Unless there is no hope that a patient will survive, the medical system does not stop caring for injured Canadians when they have reached an allotted per capita amount of spending. The same applies to the care patients receive for cancer and heart disease. Why are patients with rare disease seen differently? Relatedly, while there are few studies of adherence to medication in rare disease patients (Garcia-Muñoz et al. 2023), sufferers have every incentive to adhere to the therapy they are prescribed as they know how important it is, whereas among those suffering from many common diseases, medication adherence is frequently poor.
Of course, funding is not infinite. Someone does have to decide how much Canada is willing to pay for health care not only for rare diseases but also for common illnesses and injuries. However, this should not mean that patients with rare diseases can only be given extremely restricted access to DRDs simply because they are expensive. Spreading money more equally across different illnesses and diseases does not necessarily lead to improved care or outcomes. Canada spends more per person on health care, including prescription drugs, than most Western democratic countries (Statista 2024), yet only produces mediocre outcomes compared with peer countries (Blumenthal et al. 2025). The current restrictions on access to DRDs leads to increased direct health care costs in the future and increased suffering, which does not align with societal values or what Canadian patients want.
In an economic evaluation of the burden of rare diseases in the United States, a lack of treatment was associated with a 21.2 per cent increase in total costs per patient per year (Andreu et al. 2022). In addition, the cost for 8.4 million patients in the US affected by 373 rare diseases in the analysis was estimated to be $2.2 trillion per year and, using this estimate, the societal responsibility for all known rare diseases could be $7.2 trillion to $8.6 trillion per year in the US. Thus, denial of therapy has major costs down the road.
Canada could regulate large price reductions to make the cost of DRDs more acceptable, but this would lead to manufacturers deciding not to market their drugs in this country (Kanavos et al. 2019). We need public and private drug insurers to craft appropriate strategies with developers to make DRDs accessible to patients because, despite current discoveries, only about five per cent of rare diseases are treatable. There is a large unmet need for scientific discovery and drug development for rare diseases.
National Strategy for Drugs for Rare Diseases
The federal government has launched a National Strategy for Drugs for Rare Diseases (Canada 2024) – focusing on drugs is not a comprehensive strategy for the treatment of rare diseases – and in 2019 committed $1.5 billion over three years to “increase access to, and affordability of, effective drugs for rare diseases.” In March 2023, the government launched the first phase of the strategy, which it said would help increase access to effective DRDs and make them more affordable for patients; it would also focus on supporting patient outcomes and investment in innovation. The federal government’s approach has been to sign bilateral funding agreements with individual provinces and territories selecting drugs from a common list (Canada 2025). The list is thought to ultimately consist of 12 DRDs, but only seven are currently specified. The choice of the DRDs is based on the government’s perception of whether they are conducive to real-world evidence collection to support later reassessment of reimbursement status.
The seven current DRDs are:
- Axicabtagene ciloleucel (Yescarta) for follicular or diffuse and high-grade large B-cell lymphoma – an aggressive type of non-Hodgkin lymphoma.
- Belzutifan (Welireg) for Von Hippel-Lindau disease – a rare, inherited disorder characterized by tumors and cysts in various organs.
- Epcoritamab (Epkinly) for diffuse large B-cell lymphoma.
- Mogamulizumab (Poteligeo) for mycosis fungoides and Sézary syndrome (types of cutaneous T-cell lymphoma).
- Lumasiran (Oxlumo) for primary hyperoxaluria type 1, which causes production of excessive oxalate leading to kidney stones, kidney failure, and potentially systemic organ damage.
- Selumetinib (Koselugo) for neurofibromatosis type 1, also known as von Recklinghausen’s disease, which causes tumors to grow along nerves.
- Palovarotene (Sohonos) for fibrodysplasia ossificans progressive – a rare genetic disorder characterized by the formation of bone outside the skeleton that restricts movement and can cause severe disability.
For some of these drugs, the number of new potentially eligible patients is small, while for others it is quite large.
As of June 2025, agreements have been signed with all 13 provinces and territories. Each agreement requires 50 per cent of the funding to be spent on the designated DRDs by year three. Quebec, which has its own rare disease policy (Jospé, Champagne, and Lemelin 2022), signed an agreement to receive funds to cover drugs not tied to the common list.
Table 1 shows which of the seven DRDs the other provinces and territories have chosen to include in their agreements. Only four have signed for six or seven DRDs, while three others and all three territories have signed for four or fewer DRDs. Using estimated incidence rates, the potential number of patients who might be prescribed the drugs, excluding Quebec, is 5,462 per year. However, not every patient will be an appropriate candidate for therapy due to factors such as the stage of disease at diagnosis, the reimbursement criteria in a particular jurisdiction, and the patient’s general health.
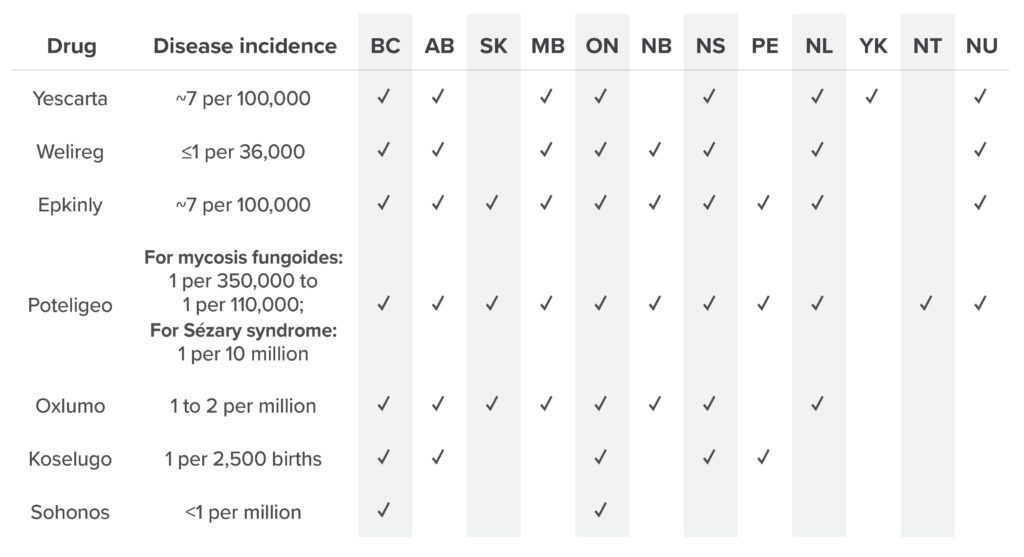
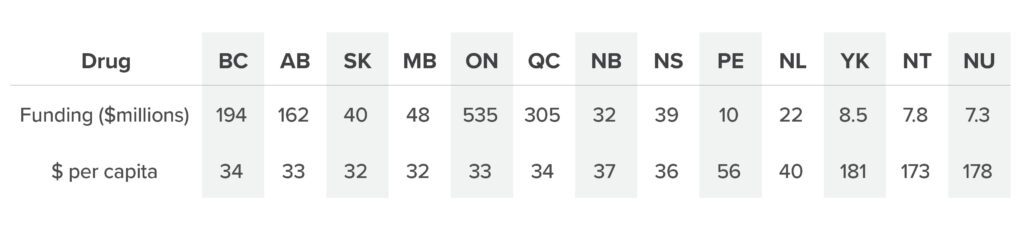
Table 2 shows how the $1.5 billion is distributed. The amount per capita is similar in eight provinces irrespective of the number of DRDs in their agreements. The per capita funding is higher in Prince Edward Island and Newfoundland and Labrador and much higher in the three territories, likely taking into account their smaller populations. The diseases that the drugs treat don’t necessarily occur equally distributed across the country, but one has to wonder whether the higher per capita funding for these provinces and territories is also intended to assist with their poorer formularies.
The current process is slowly taking baby steps towards addressing what is a significant issue of inadequate and inequitable access to DRDs. As it is currently being implemented, what the federal minister of the day announced as an initiative to reduce the wide variation in screening, diagnosis, and treatment is in fact making the situation worse by perpetuating inequitable access. It is unclear how long the funding will continue, or whether it will increase as more DRDs are added (adjusted for inflation in health care costs and economic growth).
A sustainable framework for access to new DRDs in Canada should be a lot more comprehensive and include such features as:
- A federal orphan drug designation process and a Rare Disease Act that would provide both a legal framework and intellectual property and data protection in the form of financial incentives, such as research promotion funds, targeted tax benefits, and regulatory fee reductions, to encourage innovators to make large investments in small market drug opportunities and launch new DRDs in Canada (Rawson and Adams 2022; 2023).
In the United States, the Food and Drug Administration has at least five programs to encourage developers to bring new therapies to patients who need them. Other countries have incentives to encourage research, development, production, and launch of DRDs (Gentilini, Neez, and Wong-Rieger 2025; RAREi 2024). Not only does Canada have no program or legislation to provide incentives for new DRDs, but it also has a more limited protection of intellectual property and commercial drug data than peer countries. Health Canada has a priority status review program that provides faster approval with the same level of scrutiny and a program that allows for conditional approval in a shorter time for oncology drugs but can only cope with a limited number of priority reviews at a time. Health Canada claims to be world-class, but its lack of incentive programs tells a different story. The regulator repeats the work of US and European regulators who are truly world-class, but later and after the fact.
- A consistent funding approach that would ensure timely and equitable patient access to DRDs.
The federal government’s pledge of $1.5 billion over three years is a start, but funding needs to continue and increase to cover more DRDs. Five hundred million dollars a year may sound like a lot, but it a tiny fraction of Canada’s current total health care spending. Canada must increase its spending on DRDs if more are to be covered. Canada needs a national innovation fund to support rapid access to new rare disease treatment innovations – a fund modelled on the United Kingdom’s (NHS 2025) – or it must take a new approach to its national pharmacare program by topping up the coverage offered by public and private plans to ensure that expensive DRDs are available consistently without exhausting plans’ budgets.
The focus should not be entirely on the cost of DRDs but should encompass the benefits the health system would realize were it to need fewer specialist and hospital services as well as enjoy productivity benefits. A full health economics evaluation of the use of the DRDs covering all health, social, personal, and productivity benefits will be necessary to appropriately assess the effectiveness of the national strategy.
- A separate, flexible, and timely health technology assessment process tailored to specific attributes of DRDs. In estimating the cost-effectiveness of DRDs, health technology assessment must not be restricted to using a low and outdated threshold of $50,000 per quality-adjusted life-year, a figure first adopted by Canadian health technology assessment in the 1990s.
The current process treats DRDs the in the same way as it does other drugs, with the same requirement for large-scale, comparative randomized clinical trials, and the same threshold for cost-effectiveness, which doesn’t work for DRDs. Both Health Canada and Canada’s Drug Agency need to accept evidence from innovative study designs, such as adaptive clinical trials and observational data including real-world evidence, for market authorization, health technology assessments, and creative post-marketing data collection and analysis.
The federal government should take advantage of the fact that it funds most of Canada’s Drug Agency to encourage the agency to develop a customized health technology assessment review process for DRDs that reflects the unique nature of their development and stops relying on incremental, cost-effectiveness, ration-based calculations of quality-adjusted life years, which depend on a population-based comparison of potential treatments that inherently undermines the value of the personalized treatments that are necessary for addressing rare diseases.
- More broadly, improvements to the regulatory, health technology assessment, price negotiation, and government drug plan listing processes. Such improvements would benefit all Canadians by reducing duplicative actions and the time spent on these processes, and would give citizens earlier access to new innovative medicines.
If Canada were to mutually recognize as suitable for use in this country medicines approved by world-class regulatory agencies in the US, the European Union, Switzerland, and Australia it would eliminate redundancies and shorten the time Health Canada takes to approve drugs. In addition, access to medicines would be quicker if they were made available to patients as soon as possible after regulatory approval while health technology assessments are being pursued, which should be completed in much less time than currently. Furthermore, the pCPA should make its decisions about whether to negotiate with developers of drugs reviewed by Canada’s Drug Agency and complete negotiations within its performance standards. Government drug plans should accept medicines that successfully pass these processes and provide coverage for them within a short time. Streamlining and reducing overlapping bureaucratic processes would save both money and time and provide timely access to medicines for all Canadians.
Conclusion
Canadians with rare diseases don’t need virtue-signalling or theoretical principles (Adams, Vanstone, and Rawson 2024). Nor do they need policies and practices that stifle innovation and access to innovative medicines. They need laws, like the Orphan Drug Act and the Rare Diseases Act in the United States, which will provide the resources to motivate research into diseases and development of therapies for them, to enhance intellectual property rights, and to ensure fair and timely access to innovative DRDs that can reduce suffering and improve and even save lives. Most other developed countries have such laws. Canadians with rare diseases also need a comprehensive national rare disorder strategy – not a pseudo-strategy without any legislative backing. These Canadians should not remain orphans of the country’s health care system.
About the authors
Dr. Nigel Rawson is a pharmacoepidemiologist and pharmaceutical policy researcher. He is also an affiliate scholar with the Canadian Health Policy Institute and a senior fellow with the Macdonald-Laurier Institute as well as the Fraser Institute.
John Adams is a seasoned management consultant with a current focus on advocacy for unmet patient health needs. He has extensive experience in public policy, governance, and senior management. A frequent author and commentator on health-related public issues, he is a senior fellow at the Macdonald-Laurier Institute.
References
Adams, John, Beth Vanstone, and Nigel Rawson. 2024. “On This Rarest of Days, Commit to Support Those with Rare Diseases.” Financial Post, February 29, 2024. Available at https://financialpost.com/opinion/opinion-on-this-rarest-of-days-commit-to-support-those-with-rare-diseases.
Andreu, Pedro, Jenny Karam, Caroline Child, Giacomo Chiesi, and Gina Cioffi. 2022. The Burden of Rare Diseases: An Economic Evaluation. Chiesi Global Rare Diseases. Available at https://chiesirarediseases.com/assets/pdf/chiesiglobalrarediseases.whitepaper-feb.-2022_production-proof.pdf.
Awada, Nahya. 2025. “Access to Drugs for Rare Diseases (DRD) in Canada: A Comprehensive Review of the Provincial DRD-Specific Programs.” Therapeutic Advances in Rare Disease 6: 1–12.
Begovic, Maja. 2022. “Getting Sick to Get Better: Cystic Fibrosis Patients Worry About Access to ‘Breakthrough’ Drug.” Healthing.ca, October 5, 2022. Available at https://www.healthing.ca/diseases-and-conditions/cystic-fibrosis/trikafta-cystic-fibrosis-drug-access.
Blumenthal, David, Evan D. Gumas, Arnav Shah, Munira Z. Gunja, Reginald D. Williams II. 2025. Mirror, Mirror 2024: A Portrait of the Failing U.S. Health System. Commonwealth Fund. Available at https://www.commonwealthfund.org/publications/fund-reports/2024/sep/mirror-mirror-2024.
Canada. 2024b. “The National Strategy for Drugs for Rare Diseases.” Government of Canada. Available at https://www.canada.ca/en/health-canada/services/health-care-systems/national-pharmacare/strategy-drugs-rare-diseases.html.
Canada. 2025. “Drugs for Rare Diseases: Common List of Drugs.” Government of Canada. Available at https://www.canada.ca/en/health-canada/corporate/transparency/health-agreements/shared-health-priorities/drugs-for-rare-diseases-bilateral-agreements/common-list-drugs.html.
Canada’s Drug Agency [CDA]. 2024. Pan-Canadian Guidance for Newborn Screening: Building the Foundations for Early Detection and Diagnosis of Conditions in Support of the National Strategy for Drugs for Rare Diseases. Canada’s Drug Agency. Available at https://www.cda-amc.ca/sites/default/files/DRD/HC0079-NBS-Discussion-Paper.pdf.
Canada’s Drug Agency [CDA]. 2025. Toward a Future Pan-Canadian Coordinated Approach for Newborn Screening: A Report from the Advisory Panel. Canada’s Drug Agency. Available at https://www.cda-amc.ca/sites/default/files/DRD/HC0079-NBS_Recommendations_Report.pdf.
Canadian Institute for Health Information [CIHI]. 2024. “National Health Expenditure Trends, 2024 – Snapshot.” Canadian Institute for Health Information. Available at https://www.cihi.ca/en/national-health-expenditure-trends-2024-snapshot.
Canadian Organization for Rare Disorders [CORD] 2023. Experiences of Rare Disease Patients. Canadian Organization for Rare Disorders. Available at https://www.raredisorders.ca/uploads/Documents/CORD-Rare-Disease-Survey_Full-Report_Feb-2870-2.pdf.
Canadian Organization for Rare Disorders [CORD]. 2015. Now Is the Time: A Strategy for Rare Diseases Is a Strategy for All Canadians. Canadian Organization for Rare Disorders. Available at https://www.raredisorders.ca/uploads/Documents/CORD_Canada_RD_Strategy_22May15_2.pdf.
Chancellor, Daniel, David Barrett, Ly Nguyen-Jatkoe, Shardha Millington, and Fenwick Echhardt. 2023. “The State of Cell and Gene Therapy in 2023.” Molecular Therapy 31: 3376–88.
Chittiboina, Prashant, and Russell R. Lonser. 2015. “Von Hippel-Lindau disease.” Handbook of Clinical Neurology 132: 139–56.
Dragojlovic, Nick, Clara D. M. van Karnebeek, Aisha Ghani, Dallas Genereaux, Ellen Kim, Patricia Birch, CAUSES Study, Alison M. Elliott, Jan M. Friedman, and Larry D. Lynd. 2020. “The Cost Trajectory of the Diagnostic Pathway for Children with Suspected Genetic Disorders.” Genetics in Medicine 22: 292–300.
Esquivel-Sada, Daphne, and Minh Thu Nguyen. 2018. “Diagnosis of Rare Diseases Under Focus: Impacts for Canadian Patients.” Journal of Community Genetics 9: 37–50.
Garcia-Muñoz, Ana María, Desirée Victoria-Montesinos, Begoña Cerdá, Pura Ballester, Eloisa María de Velasco, and Pilar Zafrilla. 2023. “Self-Reported Medication Adherence Measured with Morisky Scales in Rare Disease Patients: A Systematic Review and Meta-Analysis.” Healthcare 11: art. 1609. Available at https://pmc.ncbi.nlm.nih.gov/articles/PMC10253179/pdf/healthcare-11-01609.pdf.
Gentilini, Arianna, Emilie Neez, and Durhane Wong-Rieger. 2025. “Rare Disease Policy in High-Income Countries: An Overview of Achievements, Challenges, and Solutions.” Value in Health 28: 680–685.
Glaubitz, Rick, Luise Heinrich, Falko Tesch, Martin Seifert, Katrin C. Reber, Ursula Marschall, Jochen Schmitt, and Gabriele Müller. 2025. “The Cost of the Diagnostic Odyssey of Patients with Suspected Rare Diseases.” Orphanet Journal of Rare Diseases 20 : 222.
Jospé, Dara, Jean-Raphaёl Champagne, and Alexandra Lemelin. 2022. “Minister of Health Unveils Quebec’s Rare Disease Policy.” Fasken. Available at https://www.fasken.com/en/knowledge/2022/06/minister-of-health-unveils-quebecs-rare-diseases-policy.
Kanavos, Panos, Anna-Maria Fontrier, Jennifer Gill, and Olina Efthymiadou. 2019. “Does External Reference Pricing Deliver What It Promises? Evidence on Its Impact at National Level.” European Journal of Health Economics 21: 129–151.
Khure Health. 2025. “Improving the Diagnosis of Rare Diseases: An Economic Imperative.” Khure Health. Available at https://khurehealth.ca/improving-the-diagnosis-of-rare-diseases-an-economic-imperative/.
Lapteva, Larissa, Tejashri Purohit-Sheth, Mercedes Serabian, and Raj K. Puri. 2020. “Clinical Development of Gene Therapies: The First Three Decades and Counting.” Molecular Therapy 19: 387–97.
Lech, Richard, Gideon Chow, Kamalpreet Mann, Patrick Mott, Christine Malmberg, and Lindy Forte. 2022. “Historical and Projected Public Spending on Drugs for Rare Diseases in Canada Between 2010 and 2025.” Orphanet Journal of Rare Diseases 17: 371.
Lee, Tin-Suet J., Meera Chopra, Raymond H. Kim, Patricia C. Parkin, and Carolina Barnett-Tapia. 2023. “Incidence and Prevalence of Neurofibromatosis Type 1 and 2: A Systematic Review and Meta-Analysis.” Orphanet Journal of Rare Diseases 18: 292.
Miller, Kathleen L., Lewis J. Fermaglich, and Janet Maynard. 2021. “Using Four Decades of FDA Orphan Drug Designations to Describe Trends in Rare Disease Drug Development: Substantial Growth Seen in Development of Drugs for Rare Oncologic, Neurologic, and Pediatric-Onset Diseases.” Orphanet Journal of Rare Diseases 16: 265.
National Health Service [NHS]. 2025. “Innovative Medicines Fund.” National Health Service [England]. Available at https://www.england.nhs.uk/medicines-2/innovative-medicines-fund/.
Orphanet. 2009. “Classic Mycosis Fungoides.” Orphanet. Available at https://www.orpha.net/en/disease/detail/2584.
Orphanet. 2013. “Sézary Syndrome.” Orphanet. Available at https://www.orpha.net/en/disease/detail/3162.
Orphanet. 2020. “Primary Hyperoxaluria.” Orphanet. Available at https://www.orpha.net/en/disease/detail/416.
RAREi. 2024. Finding the Missing Piece: A Vision for Rare Disease Care in Canada. RAREi: Canadian Forum for Rare Disease Innovators. Available at https://www.rarei.ca/_files/ugd/ae30f2_a92f06e8c7214ba7b20fb568146d7698.pdf.
Rare-X. 2022. The Power of Being Counted: A More Accurate Count of Rare Diseases and Steps to Getting Counted. Rare-X. Available at https://rare-x.org/wp-content/uploads/2022/05/be-counted-052722-WEB.pdf.
Rawson, Nigel S.B. 2018. “Canadian, European and United States New Drug Approval Times Now Relatively Similar.” Regulatory Toxicology and Pharmacology 96: 121–6.
Rawson, Nigel S.B., and Beth Vanstone. 2021. “Politically-Instituted Barriers Against Innovative Medicines Have a Human Toll.” Canadian Health Policy Institute [CHPI], September 9, 2021. Available at https://canadianhealthpolicy.com/opinions/politically-instituted-barriers-against-innovative-medicines-have-a-human-toll/.
Rawson, Nigel S.B., and John Adams. 2024. “Orphan Drugs Approved in Canada: Health Technology Assessment, Price Negotiation, and Government Formulary Listing.” Expert Opinion on Orphan Drugs 12: 1–11.
Rawson, Nigel S.B., and John Adams. 2025. Life on Hold: How Canada’s Drug Approval Delays Endanger Patients. Macdonald-Laurier Institute. Available at https://macdonaldlaurier.ca/life-on-hold-how-canadas-drug-approval-delays-endanger-patients-nigel-s-b-rawson-and-john-adams/.
Rawson, Nigel, and John Adams. 2022. “Suffer from a Rare Disorder in Canada? Good Luck.” Financial Post, November 1, 2022. Available at https://financialpost.com/opinion/rare-disorder-canada.
Rawson, Nigel, and John Adams. 2023. “For Drug Access, Canadians with Rare Disorders Are 40 Years Behind Americans.” Financial Post, January 24, 2023. Available at https://financialpost.com/opinion/drug-access-canadians-rare-disorders-40-years-behind-americans.
Reid, Jeremy. 2016. “Rare Disease Research Helps Us Understand Medicine for All Diseases.” Blog. BioMed Central [BMC], February 26, 2016. Available at https://blogs.biomedcentral.com/on-biology/2016/02/26/rare-disease-research-helps-understand-medicine-diseases/.
Sabatini, Marco T., and Mark Chalmers. 2023. “The Cost of Biotech Innovation: Exploring Research and Development Costs of Cell and Gene Therapies.” Pharmaceutical Medicine 37: 365–75.
Standing Committee on Health. 2019. Canadians Affected by Rare Diseases and Disorders: Improving Access to Treatment. Canada, House of Commons, 42nd Parliament, 1st Session, February 2019. Available at https://www.ourcommons.ca/Content/Committee/421/HESA/Reports/RP10349306/hesarp22/hesarp22-e.pdf.
Statista. 2024. “Pharmaceutical Spending Per Capita in Selected Countries in 2023.” [Graph] Statista. Available at https://www.statista.com/statistics/266141/pharmaceutical-spending-per-capita-in-selected-countries/.
Therrell, Bradford L., Carmencita D. Padilla, J. Gerard Loeber, Issam Kneisser, Amal Saadallah, Gustavo J. C. Borrajo, and John Adams. 2015. “Current Status of Newborn Screening Worldwide: 2015.” Seminars in Perinatology 39: 171–87.
Wang, Sophia S. 2023. “Epidemiology and Etiology of Diffuse Large B-cell Lymphoma.” Seminars in Hematology 60: 255–66.
Ward, Leanne M., Alexandra Chambers, Emine Mechichi, Durhane Wong-Rieger, and Craig Campbell. 2022. “An International Comparative Analysis of Public Reimbursement of Orphan Drugs in Canadian Provinces Compared to European Countries.” Orphanet Journal of Rare Diseases 17: art. 113. Available at https://ojrd.biomedcentral.com/articles/10.1186/s13023-022-02260-6.
Weber, Evan W., Marcela V. Maus, and Crystal L. Mackall. 2020. “The Emerging Landscape of Immune Cell Therapies.” Cell 181: 46–62.
World Health Organization [WHO]. 2025. Rare Diseases: A Global Health Priority for Equity and Inclusion. Report EB156/CONF./2. World Health Organization. Available at https://apps.who.int/gb/ebwha/pdf_files/EB156/B156_CONF2-en.pdf.
Yang, Grace, Inna Cintina, Anne Pariser, Elisabeth Oehrlein, Jamie Sullivan, and Annie Kennedy. 2022. “The National Economic Burden of Rare Disease in the United States in 2019.” Orphanet Journal of Rare Diseases 17, 1: art. 163. Available at https://ojrd.biomedcentral.com/articles/10.1186/s13023-022-02299-5.